In emergency services there is a moment most people never see.
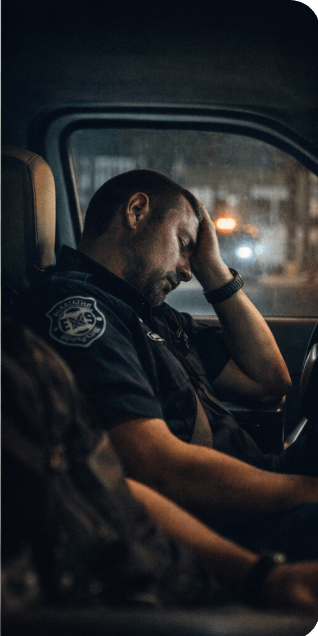
It usually happens sometime after midnight, when the world is quiet and the station lights are dim. The calls have slowed down just enough that someone finally drifts off in the Bunkroom.
Then the tones drop.
Within seconds the calm disappears. Boots hit the floor, radios crackle to life, and another emergency begins.
For many first responders, that moment repeats itself again and again over the course of a shift. Sleep comes in fragments—ten minutes here, twenty minutes there—if it comes at all.
Yet the work still has to be done.
Patients still need treatment. Ambulances still need to move quickly and safely through traffic. Decisions still have to be made in seconds.
So how do first responders manage when sleep is scarce?
The answer, in many cases, is a combination of training, teamwork, and habits built over years of long nights.
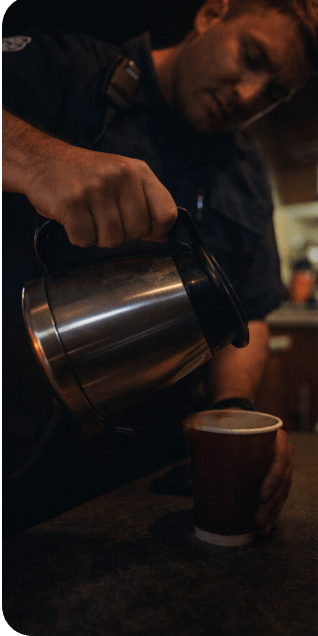
Coffee: The Unofficial Fuel of Emergency Services
Walk into almost any firehouse, EMS station, or dispatch center. You will find a coffee pot that never truly turns off.
Caffeine has become the unofficial fuel of emergency work. It sharpens focus, pushes back fatigue, and gives providers the extra edge they need when exhaustion begins to creep in.
But caffeine is a temporary solution, not a cure. It can help providers stay alert for short periods, but it cannot replace the restorative effects of real sleep.
Still, for many crews working through the night, that cup of coffee becomes a small but necessary ally.
The Power of the Partner Check
Another important defense against fatigue is something emergency services have relied on for decades—watching out for each other.
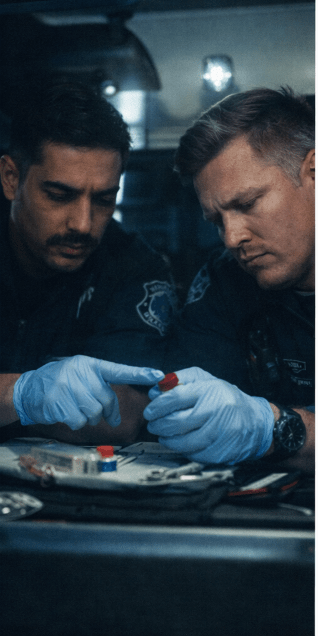
In EMS and law enforcement alike, partners often double-check each other’s work when exhaustion sets in.
One medic confirms a medication dose while the other prepares it. A partner reviews a treatment decision before it is carried out. A tired driver is reminded to pull over or slow down when fatigue becomes obvious.
These small moments of teamwork are often invisible to the public. Still, they are an important safety net inside the profession.
Experience and Muscle Memory
Years of training also play a role in helping providers function when they are tired.
Many of the most critical skills in emergency medicine are practiced repeatedly until they become almost automatic. Starting an IV, assessing a patient’s airway, or reading a cardiac monitor are actions that experienced providers perform almost instinctively.
That muscle memory helps bridge the gap when fatigue clouds thinking.
But even the most experienced provider is still human. Fatigue eventually catches up with everyone.
Humor in the Middle of the Night
One of the most common coping tools in emergency services may surprise outsiders: humor.
First responders have a long tradition of gallows humor. It’s a way of releasing tension, staying connected with coworkers, and pushing through difficult moments.
A quiet station at three in the morning may suddenly erupt in laughter. It might be over a joke, a story from a previous call, or something completely ridiculous.
That humor isn’t about disrespect. It’s about survival.
Sometimes laughter is the only thing that keeps a tired crew moving through the night.
The Quiet Drive Back to the Station
After the sirens fade, the patient is delivered to the hospital. There is often a quiet drive back to the station.
For many providers, that ride is the moment when exhaustion becomes most noticeable.
The adrenaline of the call is gone. The road stretches ahead. The body begins to remember how tired it really is.
Those moments are why conversations about fatigue are becoming more important within emergency services.
First responders have always found ways to push through exhaustion. However, the goal should never be simply to endure it.
The goal should be to manage it.
A Profession Built on Dedication
The reality is that fatigue has always been part of emergency services.
Long shifts and unpredictable calls are part of the job. The responsibility of protecting the public adds to it. This means the job will never fit neatly into a normal sleep schedule.
But despite those challenges, first responders continue to answer the call.
They rely on training, teamwork, and professionalism to carry them through the long nights.
And when the tones drop again—whether it’s midnight, three in the morning, or just before sunrise—they get up and go.
An International Discussion For Police,Fire, EMT’s, Dispatch and You!
WHEN EMERGENCIES ARRISE AND THOSE RESPONDING ARE TOO TIRED TO BE THERE
For paramedics, EMTs, and first responders, sleep often becomes the one thing emergency medicine never seems to deliver. The science is clear—fatigue affects judgment, safety, and patient care. Yet the process still runs on sleepless shifts.
When the Tones Drop at 3 A.M.: Fatigue and the Reality of EMS Life
For EMS providers, fatigue isn’t just an inconvenience or a badge of honor. It’s a real operational risk that affects patient care, provider safety, and the long-term health of the workforce. Research over the past several decades has repeatedly shown that lack of sleep slows reaction time. It interferes with judgment. It also increases the likelihood of mistakes and accidents.
You understand something the general public rarely sees if you’ve ever been jolted awake in a station Bunkroom. This happens when the shrill sound of dispatch tones rings at 2:47 in the morning. In emergency medical services, sleep often feels like something promised but rarely delivered.
Anyone who has worked long shifts in emergency services knows exactly what that looks like in the real world. The medic drives back from a call, fighting heavy eyelids. The paramedic double-checks medication calculations at four in the morning because the numbers won’t quite settle in the brain. The crew member stares at a cardiac screen, trying to push through mental fog.
Before we talk about solutions, it helps to understand how EMS developed this culture of chronic sleep deprivation. It’s also important to know why meaningful rest can be so difficult to find on the job.
Sleep isn’t a luxury. It’s a biological need that allows the brain and body to recover and operate properly. Most adults need somewhere between seven and nine hours of restorative sleep within a 24-hour period.
For EMS providers, reaching even half that amount during a shift can feel like a victory.
Research shows that the effects of sleep deprivation can be dramatic:
• After approximately 17 hours awake, a person’s cognitive performance declines significantly. It begins to resemble someone with a blood alcohol concentration around 0.05%. • After 24 hours without sleep, impairment can resemble a 0.10% BAC, well above the legal driving limit in most states. • Fatigue affects reaction speed, memory, and the ability to make complex decisions—all critical skills in emergency medicine.
Studies examining EMS providers have also revealed troubling patterns. Many report experiencing severe fatigue regularly. A significant number acknowledge that they have fallen asleep behind the wheel after finishing a shift.
For providers in the field, these statistics aren’t abstract numbers. They show up in everyday moments:
• struggling to concentrate on a pediatric medication calculation • catching yourself drifting at a stoplight on the way back to the station • taking longer than usual to interpret patient data during a call
The long-term consequences of chronic sleep deprivation can also be severe. Poor sleep has been linked with higher risks of heart disease, diabetes, obesity, depression, and anxiety. Over time, fatigue contributes to burnout and drives experienced providers away from the profession.
Ironically, other industries that rely on safety-critical decision making—like aviation and commercial trucking—strictly regulate work hours and rest periods. EMS, nonetheless, often operates under schedules that allow providers to stay on duty for 24 hours or longer.
How EMS Ended Up With 24-Hour Shifts
Many EMS scheduling practices trace their roots to the fire service.
When modern EMS systems began developing in the 1960s and 1970s, many ambulance operations were integrated into fire departments. Firefighters traditionally worked 24 hours on duty. They followed this with 48 hours off. This schedule was manageable when fire calls were relatively infrequent.
EMS adopted this structure, even though medical call volumes soon far exceeded those of fire responses.
There were several reasons the schedule remained popular:
Staffing efficiency Long shifts need fewer personnel to keep coverage.
Fewer commutes Working a 24-hour shift means fewer trips to and from work during the week. This is something many providers appreciate, especially those in rural areas.
Overtime opportunities Long shifts make it easier to pick up extra work. This increases income for providers. It also reduces hiring pressure on agencies.
Tradition Like many aspects of emergency services culture, once a system becomes established it tends to stay that way.
Other Scheduling Models
Although the 24-hour shift remains common in many departments, other models are used as well.
12-hour shifts Common in high-volume urban EMS systems. They reduce extreme fatigue but need more staff and more frequent shift changes.
Kelly schedules A modified version of the 24/48 rotation that periodically adds an extra day off for recovery.
48/96 rotations Two days on duty followed by four days off. Some providers enjoy the extended time off, but fatigue can become severe if call volume is high.
Peak-hour staffing Extra crews are scheduled during the busiest times of day to reduce workload during overnight hours.
Each system has advantages and disadvantages. The challenge for agencies is balancing staffing levels, budgets, and provider well-being.
The Reality of Multiple Jobs
Another factor contributing to fatigue is the financial reality of EMS work.
Many providers hold second—or even third—jobs to make ends meet. A medic often finishes a 24-hour shift at one service. Then, they report to another agency for extra hours.
In some cases, providers stay awake and working for 48 hours or longer. While overtime can be financially appealing, the physical and mental toll can be enormous.
Why Sleep Is So Difficult in EMS
Even when schedules theoretically allow for rest, real-world conditions often make sleep difficult.
Unpredictable call volume One shift is quiet, while the next produces a constant stream of calls.
Station environments Bunkrooms are noisy, crowded, or poorly designed for restorative sleep.
Cultural expectations In some departments, daytime naps are still discouraged despite overnight calls.
Stigma surrounding fatigue Many providers hesitate to admit exhaustion for fear of appearing weak.
The result is a workforce that often operates on minimal rest while still being expected to deliver high-level medical care.
What Agencies Are Trying
Across the United States and internationally, EMS organizations have begun experimenting with strategies to tackle fatigue.
Fatigue management programs Training and policies designed to recognize fatigue as a safety hazard.
Improved sleep spaces Some agencies are redesigning stations to create quieter, darker rest areas for crews.
Adjusted shift schedules Shorter shifts or hybrid scheduling models may reduce extreme fatigue.
Data-driven staffing Deploying extra units during peak call hours can reduce workload during overnight periods.
None of these solutions is perfect. Budget constraints, staffing shortages, and operational demands make large changes difficult for many agencies.
Still, awareness of the issue is growing.
Personal Responsibility Matters Too
While system design plays a major role, providers also have some responsibility for managing fatigue.
That means prioritizing sleep on off-days, maintaining healthy routines, and recognizing when exhaustion affect performance.
Emergency services professionals often pride themselves on toughness, but fatigue is not a personal weakness—it’s a biological reality. Recognizing its effects is part of professional responsibility.
When fatigue becomes normalized within a profession, the consequences ripple outward.
Operational efficiency declines. Morale suffers. Experienced providers leave the field.
Most importantly, fatigue can affect the quality of care patients get.
Communities depend on EMS professionals to respond quickly and make critical decisions under pressure. Those responsibilities need clear thinking and alertness—something difficult to keep without adequate rest.
Moving Forward
Fatigue will always be part of emergency services to some degree. The unpredictable nature of the job makes perfect schedules impossible.
But acknowledging the problem is an important first step.
Agencies can explore smarter scheduling, better rest environments, and policies that recognize fatigue as a safety issue. Providers can take steps to manage their own sleep habits and recovery time.
The tones will still drop in the middle of the night. That’s part of the job.
The profession can continue working toward systems. These systems protect both the providers who answer those calls. They also protect the communities they serve.
Tomorrow Part II – Running on Coffee and Commitment: How First Responders Survive Fatigue
References
Williamson AM, Feyer AM. Moderate sleep deprivation produces impairments in cognitive and motor performance equivalent to legally prescribed levels of alcohol intoxication. Occup Environ Med. 2000 Oct;57(10):649-55. doi: 10.1136/oem.57.10.649. PMID: 10984335; PMCID: PMC1739867.
Billings JM. Firefighter sleep: a pilot study of the agreement between actigraphy and self-reported sleep measures. J Clin Sleep Med. 2022 Jan 1;18(1):109-117. doi: 10.5664/jcsm.9566. PMID: 34314350; PMCID: PMC8807900.
Patterson PD, Martin SE, Brassil BN, Hsiao WH, Weaver MD, Okerman TS, Seitz SN, Patterson CG, Robinson K. The Emergency Medical Services Sleep Health Study: A cluster-randomized trial. Sleep Health. 2023 Feb;9(1):64-76. doi: 10.1016/j.sleh.2022.09.013. Epub 2022 Nov 10. PMID: 36372657.
Cox M, Cramm H. Laying the foundation: exploring the family impact of public safety personnel sleep health. FACETS. 2025;10:1-14. doi: 10.1139/facets-2025-0081
Holland-Winkler AM, Greene DR, Oberther TJ. The Cyclical Battle of Insomnia and Mental Health Impairment in Firefighters: A Narrative Review. J Clin Med. 2024 Apr 9;13(8):2169. doi: 10.3390/jcm13082169. PMID: 38673442; PMCID: PMC11050272.
Marvin G, Schram B, Orr R, Canetti EFD. Occupation-Induced Fatigue and Impacts on Emergency First Responders: A Systematic Review. Int J Environ Res Public Health. 2023 Nov 12;20(22):7055. doi: 10.3390/ijerph20227055. PMID: 37998287; PMCID: PMC10671419.
Huang G, Lee TY, Banda KJ, Pien LC, Jen HJ, Chen R, Liu D, Hsiao SS, Chou KR. Prevalence of sleep disorders among first responders for medical emergencies: A meta-analysis. J Glob Health. 2022 Oct 20;12:04092. doi: 10.7189/jogh.12.04092. PMID: 36269052; PMCID: PMC9585923.
Billings JM, Jahnke SA. Effects of a 24/48 to 48/96 Shift Schedule Change on Firefighter Sleep and Health: Short-Term Improvements and Six-Month Stability. Int J Environ Res Public Health. 2025 Nov 5;22(11):1678. doi: 10.3390/ijerph22111678. PMID: 41302624; PMCID: PMC12652382.
Be sure to follow up on emergency news and information at JEMS.
First responders are trained to notice patterns long before studies are commissioned or policies are rewritten. Sometimes danger announces itself not with a single catastrophic event, but with repetition—quiet, unsettling repetition. Over a single 24-hour period, I recorded eight separate headlines. Each headline involved police officers being struck by vehicles while working crashes or traffic stops. Eight. Different states. Different agencies. Same outcome. This situation raises a controversial and long overdue question. Are modern LED strobe lights unintentionally putting first responders in greater danger?
There was a time when emergency lights rotated. They swept. They moved with rhythm. The old beacons gave drivers something important—a visual break. A moment for the brain to process direction, distance, and motion. Today’s LED systems don’t rotate; they pulse. Rapidly.
Aggressively. Relentlessly. High-intensity strobes which floods the visual field, especially at night. Instead of guiding a driver away from danger, it overwhelms the brain’s ability to react. The result, in theory, is not panic—but fixation. The eyes lock on. The vehicle drifts toward the brightest point. Not out of intent, but neurological confusion.
Some call it “target fixation,” a phenomenon well known to pilots, motorcyclists, and tactical drivers. Under stress, humans often steer toward what they’re staring at—even when that object shows danger. Combine that instinct with modern LED strobes. These strobes flash faster than the brain comfortably processes. The warning light becomes a lure. A hypnotic point of focus. A tragic beacon.
Eight Officers Were Struck In 24 Hours. Different States. Same Strobe Style Lighting.
Is it time to ask whether modern emergency strobes are warning drivers—or pulling them in?
Within just one day, these were the headlines recorded:
• 1 arrested for allegedly driving while intoxicated after rear-ending a police cruiser on I-465
• Las Vegas police officer injured after vehicle hit while investigating a separate crash
• Effingham County deputy hospitalized after being struck by a vehicle, authorities confirm
• Police cruiser struck by car, officer injured in Naugatuck
• State trooper vehicle damaged after being hit during a traffic stop
• Norman police officer critically injured after being struck by a car on State Highway 9
• Winston-Salem police officer injured after impaired driver crashed into three patrol cars
• Waterbury man injured Naugatuck officer in hit-and-run crash
Eight incidents. One recurring element: emergency lighting designed to protect, now contributing to harm.
This is not an indictment of technology, nor a dismissal of impaired or reckless driving. Accountability still matters. But safety demands that we ask difficult questions—even when the answers challenge long-standing assumptions. If the very lights meant to warn motorists are instead disorienting them, then tradition, training, and procurement policies deserve re-examination.
Officers and firefighters shouldn’t have to stand in the road. They shouldn’t be wondering whether the light behind them is helping. They shouldn’t wonder if it’s painting a target on their back.
Sometimes progress requires us to look backward. Sometimes the old way worked better. And sometimes, the most dangerous thing on the roadside isn’t the driver who fails to slow down. Instead, it’s the light that never lets them look away.
This isn’t meant to be the final word — it’s meant to start a conversation.
If you’re a first responder, dispatcher, firefighter, EMT, tow operator, or a motorist, your experience matters. If you have ever felt disoriented by modern emergency lighting, your experience matters.
Have you noticed drivers drifting toward scenes instead of away from them? Do today’s LED strobes feel different than the rotating lights of the past? Or do you believe visibility has improved safety overall?
Share your thoughts, experiences, or observations in the comments. Respectful discussion is encouraged. If patterns are being noticed on the roadside long before they’re studied in boardrooms, it’s worth listening. Lives depend on it.
Benjamin Groff is a former police officer and radio news anchor. He has hosted programs for CNN and ABC News affiliates in Oklahoma, Colorado, and Wyoming. His career in law enforcement began in 1980 and lasted more than two decades. This gave him first hand insight into the criminal mind and public safety. Moreover, it provided him with an understanding of the human stories that often go untold. His writing draws on these experiences, blending street-level truth with a journalist’s eye for the bigger picture.
In law enforcement, some memories haunt you, especially the ones from the most harrowing nights on the job. I was an emergency dispatcher for a police department in southwest Oklahoma, responsible for dispatching fire, police, and ambulance services across five communities. Nights could get overwhelming, but one Saturday evening stands out.
Calls had been constant. Officers were busy responding to domestic disturbances, prowler sightings, burglaries, and other emergencies. In the 1980s, our department monitored Channel 9 on a citizen’s band radio, the go-to emergency frequency.
After 1:00 AM, a call cut through the static:
“Please help—we have an EMERGENCY!”
The voice was frantic. I picked up the station radio and replied, “This is Carnegie Police Department. Go ahead with your emergency traffic.”
The caller explained that a car had veered off the highway east of town, hit a ditch, and burst into flames. The driver was trapped inside. There was no time to lose. I quickly alerted the local police unit, activated the volunteer fire and ambulance lines, and relayed the details.
“Carnegie, Unit 2, be advised—a signal-82 subject is trapped in a burning vehicle near Carlin Lawrence Airport, east of Carnegie on Highway 9.”
The unit acknowledged and responded immediately. Meanwhile, I could hear the fire chief coordinating firefighters over the phone, and the ambulance confirmed they were en route.
Since the crash was outside city limits, I switched to the state’s point-to-point frequency to contact the Oklahoma Highway Patrol.
“Carnegie Police Department to Lawton OHP—rush traffic.”
The “rush traffic” designation signaled an urgent, life-or-death call. The OHP dispatcher responded immediately, and I relayed the details. Within seconds, they were alerting highway patrol units. Nearby sheriff’s deputies also began converging on the scene.
From the initial call, the first responders arrived in just over two minutes. The fire department reached the scene in under seven minutes, and the ambulance arrived by minute eight. The Highway Patrol, coming from the county seat 25 miles away, arrived about 30 minutes later.
Tragically, there was a home nearby, less than half a block from where the car crashed. The residents had slept through the commotion, unaware of the horror unfolding so close. Later, we discovered that the vehicle was registered to someone living in that house— their son. Breaking the news was a gut-wrenching moment for all of us.
The medical examiner arrived around 4:00 AM. Once the flames had subsided, investigators could finally assess the scene. The examiner determined that the driver had died on impact; the fire had not been the cause. If the driver had died from the flames, he would have shown signs of struggling for breath, but there were none. After sending the body for a complete analysis and identification through dental records, investigators believed that he’d likely fallen asleep at the wheel on his way home from a party. There was no indication of intoxication.
The smell of a burning body lingers. For days, sometimes weeks, it haunts those who encounter it. It’s one of the harshest experiences for civilians to witness, let alone the emergency responders who encounter it repeatedly. Nothing truly prepares you for a night like that, even for the most seasoned law enforcement and fire personnel.
Fire Station 12 stood proudly in the heart of the bustling city, a symbol of protection and service. Named in honor of the fusion of Fire Stations 1 and 2, it held a legacy of bravery and dedication within its walls. At its helm was Hank, the seasoned veteran who had witnessed the evolution of firefighting firsthand.
Hank’s connection to the station ran deep, rooted in the early days when he and the Little Red Fire Truck epitomized heroism. Together, they had faced the fiercest blazes and emerged victorious, earning the community’s admiration. But as time passed, the dynamics shifted, and modernization took hold.
The Little Red Fire Truck, once a beacon of hope, now stood relegated to parades and backup duty. Hank, too, found himself on the sidelines more often, overshadowed by the younger firefighters and their state-of-the-art equipment. Yet, his dedication to the station never wavered.
Fate intervened on a warm afternoon when grass fires raged, and the station buzzed with activity. A desperate call for help echoed through the halls, signaling a mother and child trapped in a burning home. Hank knew he had to act swiftly with the other firefighters tied up on distant calls.
Without hesitation, he usurped the Little Red Fire Truck, a solitary figure against the backdrop of chaos. Ignoring protocol, he raced through the streets, the vintage engine roaring with renewed purpose. Upon Hank’s arrival at the scene, flames licked at the sky, and a crowd gathered, helpless.
Undeterred, Hank sprang into action, orchestrating a daring rescue. With precision born of experience, he deployed the aging truck’s capabilities, tapping into its reservoir of courage and resilience. Hank ventured into the inferno as the flames danced menacingly, emerging triumphant with the mother and child in tow.
The neighborhood erupted in cheers, and the world took notice, captivated by the spectacle of one man and his faithful companion defying the odds. Unbeknownst to Hank, his courage had transcended local acclaim, sparking a global wave of admiration.
But amidst the accolades, Hank remained grounded, his focus unwavering. As he extinguished the last embers of the blaze, a familiar figure approached – the Fire Chief, a mix of pride and relief etched on his face.
In a candid moment, the Chief revealed the bureaucratic hurdles that had hindered the station’s effectiveness, expressing a wish for more like Hank and his beloved Little Red Fire Truck. Yet, Hank, ever humble, pondered the Chief’s words, grappling with the shifting landscape of firefighting.
In the quiet moments that followed, as Hank bid farewell to another day of service, he found solace in the familiar embrace of the Little Red Fire Truck. With a promise to uphold its legacy, he embarked on the journey home, the echoes of the day’s heroics lingering in his heart.
For Hank, retirement loomed on the horizon, a bittersweet inevitability. But as long as the Little Red Fire Truck stood by his side, he knew their legacy would endure, a testament to the timeless virtues of courage, camaraderie, and unwavering resolve.